Mental Health Impact of Disasters
Mental Health Impact of Disasters
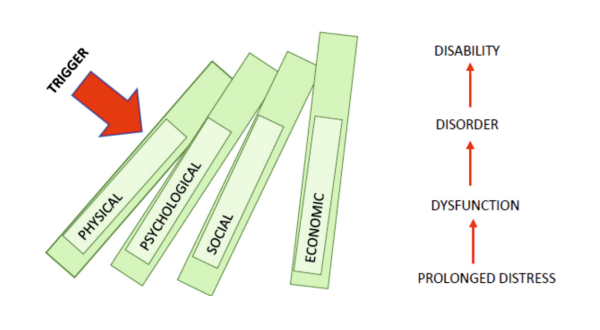 Disaster creates short-term and long-term impact on the affected community due to various reasons such as- shock from the event, loss of lives and livelihood, property destruction, lack of shelter, loss of privacy, uncertainty about recovery, bereavement, and grief etc. The impact of disaster can be broadly classified into following domains;
Disaster creates short-term and long-term impact on the affected community due to various reasons such as- shock from the event, loss of lives and livelihood, property destruction, lack of shelter, loss of privacy, uncertainty about recovery, bereavement, and grief etc. The impact of disaster can be broadly classified into following domains;
- Physical impact: The damage caused to body/physical structures or worsening of pre-existing physical condition. Examples; wound, injury, fractures, skin allergies, pregnancy complications etc.
- Psychological impact: Denotes the, emotional or behavioural reactions in response to a disaster. Examples; shock, denial, fear, anger, anxiety, grief reactions, substance dependence etc.
- Social impact: Refers to the hardship created in the family or society. Examples; displacement, migration, increase in single parent families, increase in crime and delinquency etc.
- Economic impact: Indicates the financial, property and livelihood losses. Examples; unemployment/underemployment, debt traps, loss of property etc.
Impacts of disaster are interconnected. Generally, physical, and economic impacts get larger visibility in any disasters. The impact be it physical or economic, eventually lead to a psychological impact. However, psychological impact remains under recognized. Poor awareness on mental health is one of the main reasons for poor sensitivity to the psychosocial impact created by disasters. Hence, Primary Care Doctors (PCDs) need to be mindful of the biopsychosocial impact subsequent to any disaster.
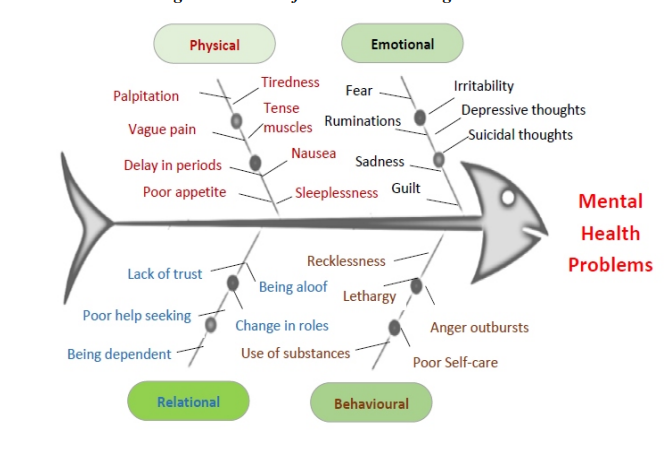
Stressful Reactions During Disasters
Stressful reactions are common in response to disaster. These reactions vary from person to person and disaster to disaster. However, it is important to note that these are the ‘normal reactions during disaster’. Every individual experiencing stressful reactions need not develop mental health complications. Yet, everybody touched by the disaster benefit from psychosocial support (PSS) and do not require medicines or psychotherapy.
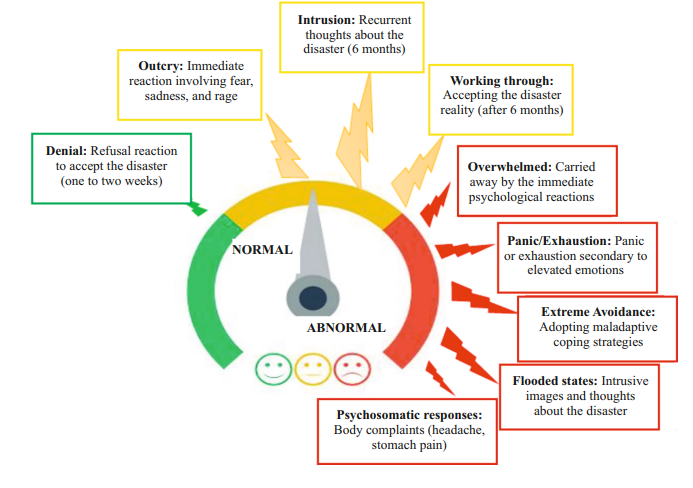
Normal and abnormal reactions post-disasters
Although disaster is a crisis situation, all the reactions to such crisis need not be abnormal. The PCDs should be able to distinguish between normal and abnormal reactions. This helps to provide focussed attention immediately and also to assess the need for referral to further specialised services as necessary.
The following tips help to distinguish such reactions;
Whether the;
- Fear, sadness, or other symptoms are persistent and prolonged
- Mental health issues are overwhelming the capacity of the individual
- Emotional problems are interfering with daily work
- Mental health issues affect the self-care or caring for others in the family
- Person is having thoughts of suicide
- Person is trying to harm self or others
- Person is being excessively angry, irritable, or violent
- Substance intoxication or withdrawal symptoms are prominent
- Individual is repeatedly seeking help
- Symptoms are not resolving even after primary care is provided
- Pre-existing mental health issues present
- Pre-existing disability present
- Extreme avoidance in participating in community activities
- Social support to an individual is poor
Common Mental Health Disorders In Disasters
The stress reactions aftermath of disasters subsides in first 1-2 weeks. If these stress reactions go beyond a month and exceeds the coping ability of the affected people, it poses threat to the mental health. The most common mental health disorders encountered by the disaster affected community immediately after a disaster includes- acute stress reactions/disorders, adjustment disorder, anxiety, depression, and sleep disorder. Depression, post-traumatic stress disorder (PTSD), and substance use disorders are the common long-term consequences of disasters. Almost 30-40% of individuals affected by disasters present with symptoms suggestive of anxiety and depression during the acute phase. The prevalence of mental health problems decreases around 10-15% by the end of 6 months after disasters.
Acute stress reactions/disorders
In response to exceptional physical and mental stress or traumatic experience caused by disaster affected individual may develop this transient disorder. Such traumatic experiences include serious threat to the safety of self or loved ones, and unexpected threatening change in the social position/network (e.g., disruption of the property and environment, multiple bereavement etc). Individual vulnerability (physical exhaustion or organic factors) and coping capacity add to the risk of developing this condition and also determine its severity. Immediately or after few minutes of getting exposed to an overwhelming stressor the person may experience shock, confusion, depression, anxiety, anger, despair, over activity, and withdrawal. None of these symptoms prevails for long. When the individual is separated from the stressful environment, the symptoms resolve rapidly within few hours. If the stress continues, the symptoms subside within 24-48 hours or at the most within 3 days.
Adjustment disorder
This disorder is the manifestation of a significant life change or consequences of a stressful life event, leading to subjective distress and emotional disturbance. Vulnerability factors serve as a major risk factor in determining the adjustment disorder. The symptoms include low mood, anxiety worry, helplessness to cope with the stressful situation and plan, and difficulty in performing daily routine. On rare instances individuals exhibit dramatic behaviour or anger outburst. Regressive behaviours such as bet-wetting, baby talk, or thumb sucking can be seen children. Following the stressful event or life change the onset occur within 1 month and the duration of symptoms does not usually exceed 6 months.
Anxiety disorders
Anxiety disorders are a spectrum of common mental disorders that include acute stress, generalised anxiety disorder, panic disorder, specific phobias, dissociative disorder, somatoform disorder, obsessive compulsive disorders, post-traumatic stress disorder etc. Common features of anxiety disorders include feeling restless, on the edge and tensed, worries about immediate future and long-term life prospects, inability to calm down or feel relaxed, headache, body aches, muscle tension, inability to get sleep, being fidgety, biting nails, pulling hairs, excessive consumption of news, completely avoiding any news, availing medical care repeatedly and seeking reassurance.
Sleep disorders
Sleep in general is disturbed in people affected by disasters due to change in environment, unsafe surroundings, loss of privacy, fear, anxiety and depression etc. Sleep disturbances are usually characterised by difficulty falling asleep, waking up multiple times in the middle of the night, experiencing nightmares and getting up early than usually intended. Persistent sleep issues may lead to poor attention and concentration, poor immunity and can interfere with daily work. Daytime sleep may lead to industrial, work place and road accidents.
Depressive disorders
Depression is one of the common mental disorders during both the acute and chronic phases following disasters. Depression is characterised by pervasive low mood (feeling sad throughout days/weeks), losing interest in any activity including previously pleasurable ones, easily feeling tired, poor sleep and appetite, decreased interaction with people, crying spells, guilt, feeling hopeless about future, death wishes and suicidal thoughts/acts. However, during the acute phase, it is to be noted that many individuals may present with a mixture of both anxiety and depressive features. Generally, 2 weeks of symptoms manifestation is required for the diagnosis of depression. Shorter periods may be reasonable if symptoms are unusually severe and of rapid onset.
Substance use disorders
Alcohol and tobacco are the commonly used substances. Based on the availability, individuals may initiate the use of alcohol/tobacco as a coping mechanism to get relieved from the stress, tension and to get sleep. Individuals previously using the substances may increase their use. Because of the severe withdrawal symptoms (headaches, nausea, tremors, anxiety, hallucinations, and seizures etc), use of alternative forms and illicit liquor may occur where alcohol is unavailable. Characteristics of substance abuse are: craving/increased urge to use the substance, ignoring other pleasures for using substance, using the substance despite knowing the harm, tolerance, withdrawal symptoms, when they repeatedly fail to stop their habit, etc.
Post-traumatic stress disorder
This disorder manifests within 6 months of a traumatic event of exceptional severity. The typical symptoms include reliving the trauma from the intrusive memories (flashbacks), daytime imagery, or dreams, emotional detachment, numbing of feeling, unresponsiveness to surroundings, anhedonia, and avoidance of stimuli that might arouse recollection of the trauma are often present. Rarely, there may be dramatic, acute bursts of fear, panic or aggression, triggered by stimuli arousing a sudden recollection and/or re-enactment of the trauma or of the original reaction to it.
Last Modified : 11/29/2023
Tips for handling mental issues during pandemics/d...
Ministry of Social Justice & Empowerment's 24x7 To...
This topic provides information about the importan...
MANODARPAN initiative of Ministry of Education is...